In their BSE Working Paper (No. 1103), “Education and Gender Differences in Mortality Rates,” Cristina Bellés-Obrero, Sergi Jimenéz-Martín and Judit Vall-Castelló investigate whether education equally affects adult mortality of men and women, at a time of increasing gender equality and women’s greater access to economic opportunities.
Gender, education, and mortality
A well-documented universal phenomenon is that, in comparison to men, women generally have a lower mortality rate and a higher overall life expectancy. However, the size of this gender gap has not remained constant over time. For instance, evidence shows a shrinkage of the gender gap in mortality rates in OECD countries.
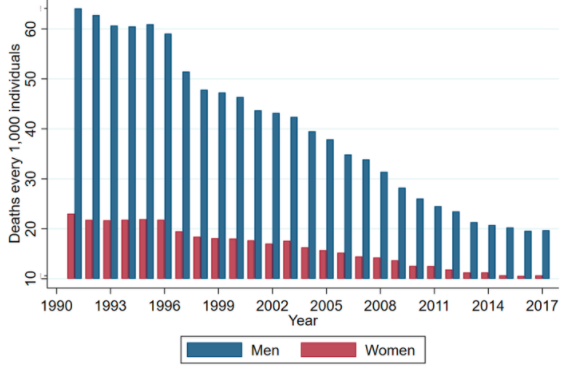
Figure 1 depicts the evolution of female and male mortality rates in Spain since 1990. Whereas in 1991 the gender difference in mortality rates for individuals aged 30-45 was 40 deaths per thousand individuals, in 2016 this difference was only 20 per thousand individuals.
Figure 1. Evolution of the mortality rate by gender in Spain
But what is behind this gender gap in mortality rate? Previous studies have explored as one possible explanation gender-specific health behaviors. Also, the effects of education on overall mortality have been extensively explored whereas gender asymmetries in the health benefits of acquiring further education have not. The authors’ contribution to the literature is, therefore, to analyze the interaction between gender and education in adult mortality.
To do so, they explore the effects of a reform introduced in Spain in 1980 that raised the legal working age from 14 to 16, while the school-leaving age remained at 14 until 1990. This scenario offers a quasi-natural experiment to estimate the effects of the reform in gender-specific mortality rates.
Understanding the Spanish worker reform and its context
Before the reform, both the earliest age for leaving school and the minimum working age were set at 14 years. This meant that individuals born at the beginning of the year were legally entitled to work before finishing their final year of primary education, while individuals born at the end of the year reached the legal working age only after completing this final year. In 1980, when the legal working age rose to 16, this difference in incentives between those born at the beginning of the year and those born at the end disappeared. The following chart illustrates these different choices depending on an individual’s month of birth before 1980.
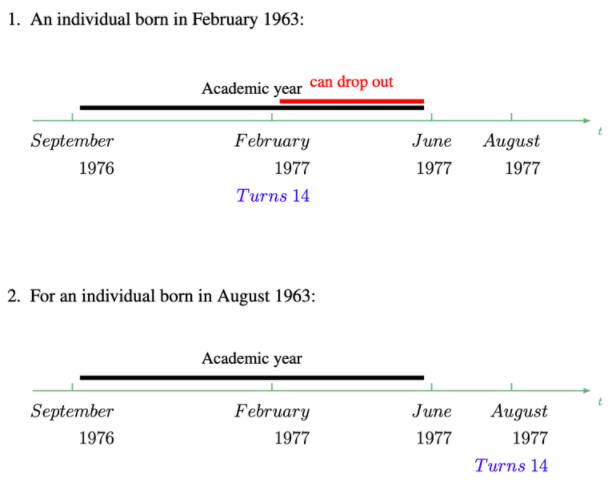
Hence, before the reform two individuals born in the same year but in different months faced different incentives to stay in the educational system during the final year of primary education: those born at the beginning of the year had fewer incentives to complete their primary education compared to others born at the end of the year. The 1980 reform eliminates these differences in incentives since all individuals, regardless of their birth month, had the same incentives to finish primary education, as now they could not work until they were 16.
Education and mortality
The paper exploits this difference in incentives between individuals born in the first months of the year and those born in the last months of the year before and after the reform to identify the causal effect of a child labor regulation on adult mortality rate.
In a previous study, the authors focus on the education and labor market impacts of this child labor reform. They show that the reform increased the probability of girls and boys finishing primary education by 1.3 percentage points (10%) and 1.2 percentage points (7.4%), respectively. At the same time, the reform decreased the number of treated girls (boys) not attaining optional secondary education by 1.2 percentage points or 2.7% (1.6 percentage points or 3.2%). These results show that restricting child labor effectively increased the educational attainment of the individuals in question.
The current paper extends their previous work by analyzing the reform’s effects on long-term mortality rates. The authors find that the reform, through its effects on education, decreased mortality of young men and women (aged 14-29) by 6.3% and 8.9%, respectively. Surprisingly, they also find that the mortality rate among prime-age (30-45) women increased by 6.3%, an effect driven by an increase in the mortality rate due to HIV (11.6%), and diseases of the nervous and circulatory system (8.7%). In fact, they find that women affected by the reform had a higher probability of consuming alcohol and of having taken an HIV test, compared to women not affected by the reform. This unexpected effect is related to the social context in Spain at the time of the reform.
Shedding light on the Spanish social context
The contextualization of the reform is crucial for interpreting the results. Spain’s Workers Statute was enacted in 1980, just a few years after the end of Franco’s dictatorship. In 1980, the country’s levels of educational attainment, child labor, and women’s social development were closer to those of a middle-income country. On the one hand, 16.19% of boys and 12.71% of girls in 1965 (last cohort not affected by the reform) did not complete their compulsory education. On the other, 49.3% of boys and 43.8% of girls in the same cohort did not finish upper secondary education.
A large percentage of the Spanish population entered the labor market at a very young age. Before 1980, around 40% (15%) of boys and 30% (10%) of girls were already working by the age of 15 (14). Moreover, health risk factors were peaking during this period; in particular, substance abuse and car accidents were at, or about to reach, a record high. Furthermore, the level of social development for those cohorts born between 1940 and 1960 was substantially different according to gender.
During the dictatorship, Spain was a male-dominated society, with women’s rights generally ignored or suppressed. This meant that very few women had access to higher education, and women’s labor market participation rates were low. For instance, in 1975 only 27.9% (34.5% in 1985) of working-age women in Spain were actually participating in the labor market. The end of the dictatorship raised the level of gender equality and improved women’s access to economic opportunities.
This gender equalization process led to a convergence of health risk factors (e.g., smoking, drinking, taking drugs, and sexual promiscuity) for both men and women. Among the cohorts of women unaffected by the reform, better educated women smoked more than women with less education. This inverse gradient for Spanish women was gradually reversed among the cohorts of women born after 1980, when the country’s gradient begins to mirror that of more developed countries, with less educated women recording higher smoking rates.
The paper’s results thus help explain the closing of the life expectancy age gap between women and men in Spain, which has narrowed by 1.5 years over the past twenty years. Furthermore, the findings are consistent with a recent strand of literature that reports differential effects of education on mortality by gender.


