Early health shocks in life have negative consequences, as they are likely to affect children’s human capital accumulation, education, and productivity. Events such as pandemics, famines, wars and radioactive emissions can create those shocks. Nevertheless, few studies focus on the factors compensating early life shocks. In their Barcelona GSE Working paper (No. 1068) “Mothers’ Care: Reversing Early Childhood Health Shocks through Parental Investments,” Cristina Bellés-Obrero, Antonio Cabrales, Sergi Jiménez-Martín and Judit Vall-Castello detect one of those compensating factors. They focus on the causal effect of a child labor regulation on the short- and long-term health of affected individuals’ offspring.
The authors empirically show that a child labor reform that took place Spain, which increased the general level of education, damaged their male children’s health at delivery. They find that male babies from more educated mothers have worse perinatal health outcomes, such as lower birth weight or low maturity. Although one would expect that such a deterioration of infant health at birth would persist in the medium and long term and would affect children’s health, they detect that there is a compensation mechanism. The long-term reversal is achieved through maternal vigilance.
Child labor reform in Spain
In 1980, a new child labor regulation (Law 8/1980) was enacted. This law changed the minimum legal age to work from 14 to 16 years old in Spain, while keeping the compulsory schooling age at 14.
At the time of the enactment of this law, primary education finished in the year students turned 14 years old. Before the new law, students born early in the year reached the minimum legal working age in their last year of primary education. This created an incentive for them to leave school before completing primary education. Students born during the last months of the year were not old enough to work legally before finishing school since they are not 14 years old yet. Hence, they had no reasons to abandon early primary education. Then, before the reform, individuals born at the beginning of the year should have a lower probability of finishing primary school than individuals born at the end of the year. After the reform, this difference in incentives disappear. After 1980, all individuals have the same incentive to finish primary education, as they were not able to work until age 16.
Data and estimation strategy
The authors perform a within-cohort difference-in-difference strategy to identify the effect of the reform on the short and medium-term health of the affected individuals’ children. They compare children whose mothers were born at the beginning of the year with children whose mothers were born at the end of the same year.
They use administrative data from the birth certificate records at the Spanish National Statistics Institute restricting the sample to first births of Spanish women born between 1961 and 1971 in order to examine the short-term effect of the child labor reform on the affected women’s offspring infant health outcomes. Their final sample has 2,493,107 first births. In addition, they use the 2000 wave of the European Community Household Panel and three waves (2003, 2006 and 2012) of the Spanish National Health Survey to examine the medium-term effects on the health of the women’s offspring.
Using least squares estimation, they regress the infant health outcome on a dummy variable indicating that the mother is born before or after the regulation, birth year dummies for mothers, calendar year and region fixed effects. When examining the medium-term effects of the reform, they also add a term for the child’s age to the equation. The main effect of the reform is identified by the coefficient of the interaction between the post-reform and treatment dummy variable.
Effect of the child labor reform on infant health in short and medium term
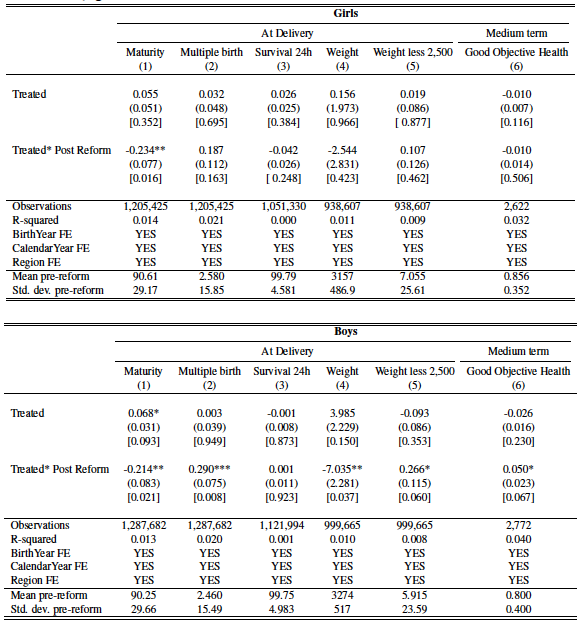
Table 1 shows the effects of the reform on infant health outcomes for all children differentiating by gender. As can be seen from the table, the main fact they find is the prominent differential impact of the child labor reform on infant health at birth, which is negative for boys only.
Firstly, they show that the reform had an effect over the probability of having a child born with less than 37 gestational weeks, which is very similar for boys and girls. Namely, after the reform, the child of a woman, no matter if it is a boy or a girl, born at the beginning of the year has a 0.234 or 0.214 percentage-point higher probability of being premature. The remaining effects of reform over the health of children mostly differ for boys and girls. The reform caused women born at the beginning of the year to have boys that weighed 7 grams less, on average, compared to boys of women born at the end of the year.
Given the previous conclusion from the medical literature, that being born with less than 2,500 grams is correlated to adverse health and developmental outcomes for children, the authors claim that the reform could have affected children’s health in the medium term if nothing is done to compensate for it. Yet, when they examine the medium-term effects of the reform over children’s health (which can be seen in the two last two columns of Table 1), the objective good health status is affected in the opposite way. While girls’ objective health is still not affected by the reform, boys from mothers affected by the reform had a 4.8 higher probability of having a good objective health. Hence, there should be a mechanism that compensated for the former negative impact.
The mechanism
The authors investigate a potential mechanism for achieving the reversal effect: maternal vigilance. More explicitly, parents can contribute to a better health by ensuring their offspring make lifestyle choices that are more conducive to good outcomes. They can also invest in other preventive measures, like taking the children more often to the doctor.
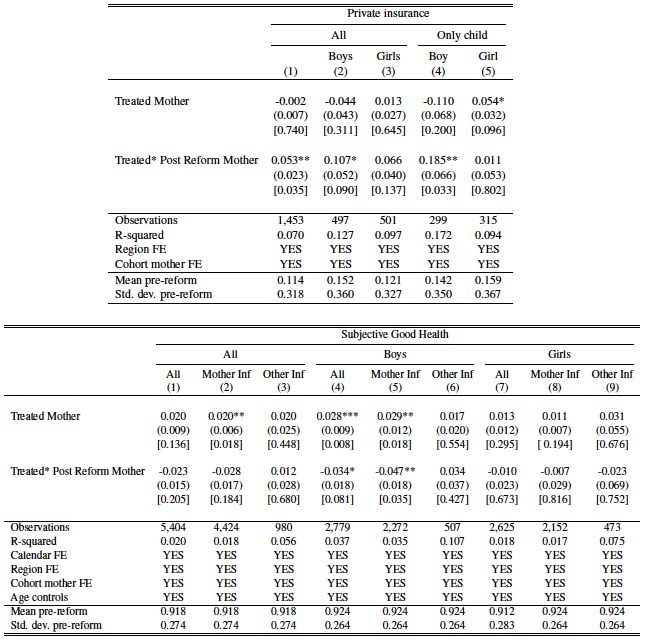
The results from Table 3 show that the boys born from mothers affected by the reform have a 3.4 percentage points lower probability of having subjective good health, while the reform had no significant impact on girls’ subjective health. The authors infer that this clearly would have triggered a larger preoccupation by mothers about their male offspring’s health. This is further reinforced by their finding that boys of treated mothers have 10.7 percentage points higher probability of having private insurance.
The picture that emerges is one of mothers who had smaller, more fragile, boys, and who still worry more about them at age 15 even if, objectively, their health does not seem to differ from that of girls. Thus, they put a lot of care, like providing expensive private insurance, to guarantee they have a positive health status. That, in turn, leads to a reversal of the negative effects at birth of the aforementioned reform.



